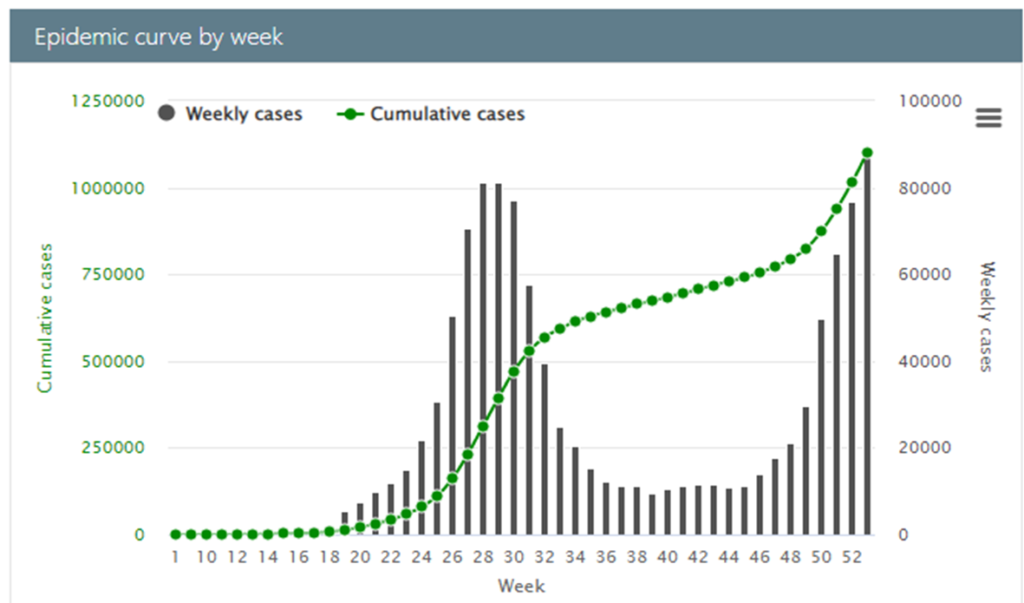
We still don’t know much about the omicron variant. Based on outcomes in South Africa, it does seem to be highly contagious. Omicron is clearly the culprit behind rapidly increasing case counts across that nation. Please see chart below. The European CDC is saying, “The evidence from the initial cases of this new variant that has been collated from around the world is limited, but suggests that the Omicron VOC [variant of concern] may be associated with higher transmissibility than the Delta VOC…”
It is too early to discern the virulence of the variant or the ability of the variant to elude current vaccines.
The variant seems to have initially emerged among clusters of unvaccinated people in their late teens and twenties (with more robust immune systems) who have mostly presented with “mild symptoms.” There are examples of breakthrough cases involving vaccinated persons, but this is also true of previous variants. It will still be awhile until we have indisputable virologic and/or epidemiologic evidence of a substantive deterioration in current and prospective vaccine defenses. The CEO’s of Moderna and Pfizer seem to take different angles on this known unknown.
In a late-breaking analysis, South African researchers have found, “Population-level evidence suggests that the Omicron variant is associated with substantial ability to evade immunity from prior infection.” This is unlike outcomes for prior variants. Immunity resulting from prior infection is different than immunity facilitated by vaccination. The researchers note, “The vaccination status of individuals with suspected reinfections identified in this study was unknown.”
We may have an early data-driven sense of virulence by next week. Given vaccination levels in South Africa, it is likely to take more time to accurately assess vaccine efficacy related to omicron using epidemiological methods. We may have virological results by mid-month.
The WHO has stipulated, “Persons who are unwell, or who have not been fully vaccinated or do not have proof of previous SARS-CoV-2 infection and are at increased risk of developing severe disease and dying, including people 60 years of age or older or those with comorbidities that present increased risk of severe COVID-19 (e.g. heart disease, cancer and diabetes) should be advised to postpone travel to areas with community transmission.”
I am an apparently healthy person over sixty years of age. This afternoon I will receive my third-jab booster. The WHO’s advice is a bit convoluted, but in any case I have concluded that given current uncertainties I can reduce the risk to myself and the risk I can present to others by minimizing my circulation. Easy enough for me. Not so easy for others. When discretionary circulation is avoided, the risk of non-discretionary circulation is systemically reduced. When circulation is necessary then being vaccinated, avoiding crowds, and minimizing nose-and-mouth proximity are helpful ways to mitigate individual risk while reducing the chance of unsustainable demand for local healthcare services.
Omicron is an additional uncertainty in a risk context already plenty treacherous, especially for those with preexisting vulnerabilities. So, we each do what we can to reduce the circulation of viral disease and preserve flows of food, pharmaceuticals — and even fun — while we wait for clear evidence of omicron’s threat profile.